The Health Informatics Service (THIS) has been at the cutting edge of NHS digitisation since its inception more than 20 years ago. Its work for its host trust, the Calderdale and Huddersfield NHS Foundation Trust (CHFT), is helping to make it one of the most ‘digitally mature’ and ‘paper light’ trusts in the UK.
Its work often involves collaborating with suppliers and manufacturers of medical equipment and systems, such as when it created a link between CHFT’s drug prescription system, hosted on EMIS software, and its Electronic Patient Record (EPR), hosted by Cerner Millennium. The first-of-type solution across the NHS removed the need for duplicated tasks between two standalone systems.
Another asset in THIS’ portfolio is the innovative work of its six-strong web development team, which scopes, develops and delivers bespoke digital solutions for CHFT’s two main hospitals, The Huddersfield Royal Infirmary and Calderdale Royal Hospital, and other NHS bodies and services in the region.

One of its latest achievements is the development of a new, bespoke Medicine Management Assurance Audit (MMA) system for CHFT’s hospitals, replacing what was a time-consuming, admin-heavy, paper-based way of working.
An MMA is an annual audit for each of the hospitals’ 60 wards/departments, to provide assurance that safe medicines management standards and policies are being met.
Karen Austin, CHFT’s Lead Nurse, Medicines Management, says:
“The yearly MMA was developed to give assurance that medicines management standards are being met on wards and in departments. It showcases good practice and highlights areas of non-compliance that require assistance to achieve compliance in any of the defined safe practice areas. In the past, the MMA had proved to be a clunky process which was reliant on audits to be completed on paper, scanned to the next person, signed, scanned to the next person and so on.”
Improving patient safety
An MMA increases accountability for the baseline safety of patients on each ward/department. Its scope includes:
- The safe storage of all medicines – ambient, refrigerated, frozen and warmed for intravenous fluids.
- Key safety and security issues.
- Patient Group Directions that ensure staff on wards/departments are competent and authorised to supply and administer medicines.
- The safe handling of pharmaceutical waste.
- The safe management of controlled drugs.
- Medicines management staff knowledge.
Rebecca Wootton is THIS’ Web Development Team Leader who managed the project. She says:
“It's all about the safety of the wards and departments and ensuring that everything is covered off annually.
For example, are the refrigerators at the correct temperature for the medicines being stored in them? Are medicines being stored securely? Is the correct paperwork for Patient Group Directions being used to make sure the staff members in that area are authorised to give out the drugs? Are they disposing of their waste correctly?
It all provides reassurance that all of this is being taken care of and not pushed to one side. It was quite easy for paper to be lost, or put in a drawer and forgotten about, or for somebody to say they’d done something when they hadn’t.”
The problem and a time-saving benefit
Previously, each printed MMA report was 12 pages in size and required sign off by the auditor, ward/department manager and the ward/department before it reached the Associate Director of Nursing (ADN), to check the action plan and finally sign off or return for adjustment.
Rebecca Wootton:
“People wouldn't know where in the whole scale of things the process was up to. They could say that they were going to do certain actions and then the ADN might not be comfortable that would rectify the problem. So, then there would be more back and forth, which was paper passing, or emailing, and things could get pushed to one side.”
It proved to be a laborious process as action points were highlighted, fed back to the ward/department and then actioned, before being fed back up the line of management for approval or further direction. In practice, the process was found to lack transparency, while the progress of each audit and its recommendations were not always clear to each of the protagonists. It needed simplifying, clarifying and expediting.
Karen Austin:
“Achieving turnaround of a fully signed off audit within a month of an audit being completed, was never achieved. It was often many weeks and sometimes months later that audits were fully signed off. This rendered the audit ‘out of date’ by the time it was finally signed off. Digitising the process was the only way forward to complete the audit fully in ‘real time’.”
It is estimated the new web-based system is saving each person in the audit trail at least an hour, in addition to time saved on photocopying, scanning and emailing – which usually equated to 10 minutes per action point. So, for example, if an MMA is processed by four people for each of the 60 wards/department, that equates to a time saving of 240 hours in total.
Other major benefits include:
- Auditors, no longer print off the documentation, scan and forward it once the initial audit has been undertaken so the action plan can be added by the ward/department manager/. Later signatories no longer have to print off before they add their comments and signatures and then printing and rescanning again before attempting to store the final, fully signed off version
- Ward/department managers/s and ADNs can log into an MMA and update it any point, rather than waiting for the paper copy to land on their desk.
- Lead Nurse, Medicines Management, no longer has to spend hours cross referencing, chasing results and planning follow up audits and support to wards/departments
Transparency for everyone
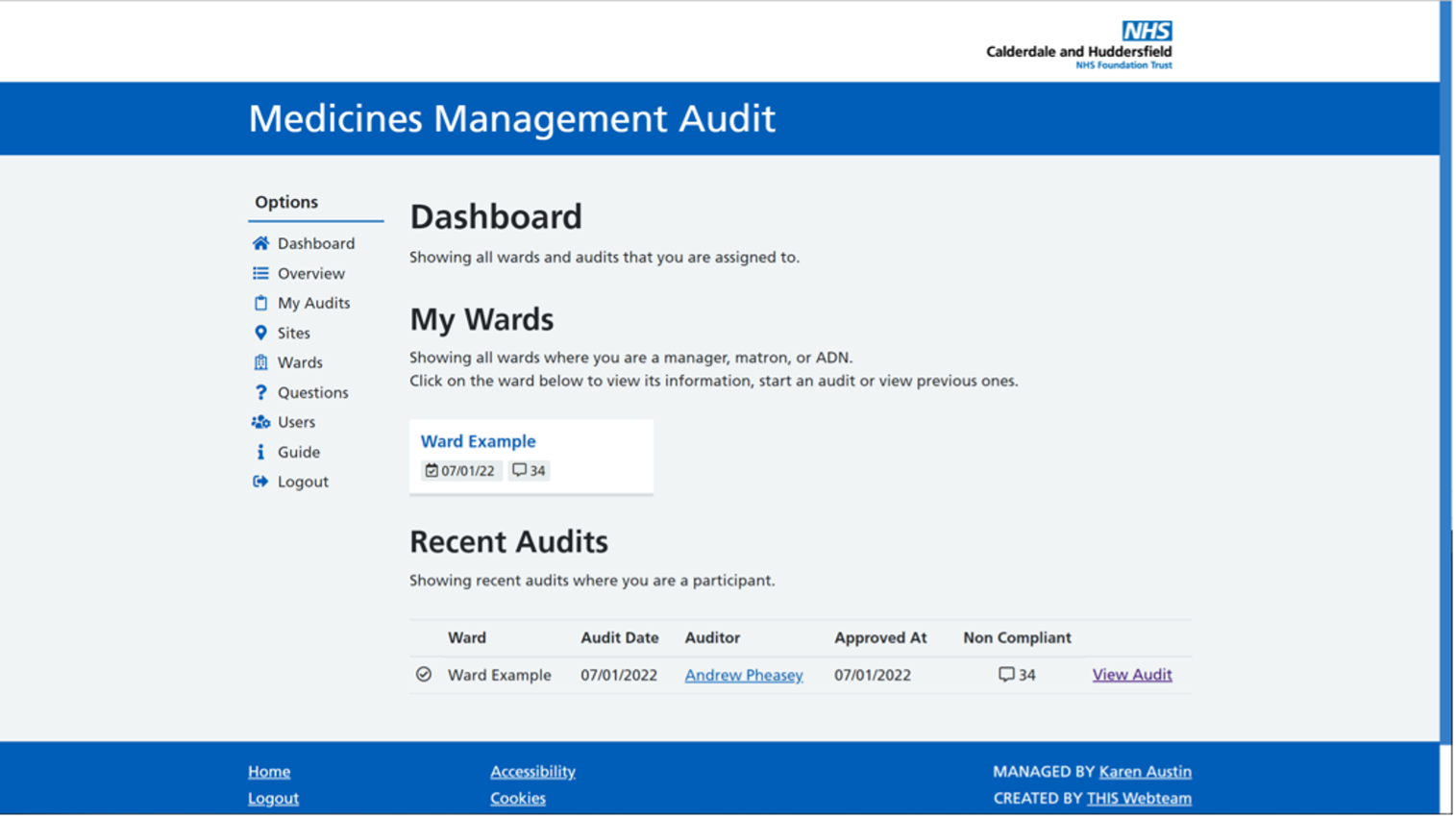
The new web-based system provides total transparency for everyone within the MMA cycle, portraying headline information on a dashboard-style home page, an example of which is pictured below.
Rebecca Wootton:
“It provides access to all the wards and departments, so with 60 of them across both sites, it is much easier to keep track of what is happening where. The users can see when the last audit was completed, how many actions they had, and make sure all the audits have been completed for that year, and how many non-compliances there have been.”
The information can be curated to show trends and year-on-year variances, to provide improved visibility for everyone in the audit trail, especially for wards/departments showing the same non-compliance issues for three consecutive audits.
The system is accessed via each user’s active directory account linked to their hospital account, which means they can only gain access while employed by the trust. It is based on an email notification system, so anyone included in the audit trail receives update reminders every time something is actioned, with emails on the day and reminders at weekly intervals until all tasks are completed.
Karen Austin:
“The process of populating (an MMA) with auditor, manager, and ADN names is a simple process and notifications are ‘fired’ via email at fixed intervals. If anyone has not in essence ‘done what they are required to do’ within the audit timeframe, reminders are fired. As system manager, I have a full overview and can monitor completion from start to finish.
A system guide is available which outlines roles and responsibilities and what access has been given to those involved in the audit. Audit questions, names etc. can be changed, added or removed quickly, which ensures only the most up-to-date audits can be accessed.”
Rebecca Wootton adds:
“Every audit can be downloaded if someone does need a paper copy, but it is very simple to view it on screen and go through all the key questions being asked, and whether the answers were found to be compliant. If they’re non-compliant, it shows a comment as to why it was marked that way and the action that has been highlighted to rectify the situation going forward.”
The plan now is to monitor the system over the next two to three years to see if other beneficial processes can be added.

A marathon not a sprint
Creating a bespoke, new system is a marathon not a sprint for THIS’ web development team. The MMA project spanned almost two years from inception to business as usual.
Rebecca Wootton explains:
“Because of the nature of the teams and departments we deal with, they've all got their day-to-day work to complete, and obviously clinical priorities take precedence. Sometimes we have to wait to agree an appropriate time to pilot a project so that it's not putting too much pressure on day-to-day responsibilities.”
All projects follow a similar process and align with the Prince2 project management principles, which are followed by THIS’ Project Management Office, and an agile, iterative way of working called the Dynamic System Development Method (DSDM). The steps include:
- Project request – this comes from the person whose idea it is to improve a system or process. It then prompts an investigation to ensure the trust doesn’t already have a similar system in operation.
- Project documentation - gathering background information about the current process and setting out goals that be quantified as KPIs when the project is complete.
- Scoping – the developers turn the background information and goals into tasks.
- In-house testing – the regime takes in baseline functionality and then ‘look and feel’. From there, it goes to a project lead to make sure the would-be users are comfortable with the changes.
- Pilot site – in the MMA project the pilot stages were completed on two wards suggested by the Lead Nurse, Medicines Management, who knew they would be comfortable collaborating in a digitally forward-thinking way.
- Launch – full roll out, planning for business as usual and training support for approximately six weeks.
- Final lessons learned – taking in feedback from the developer(s) and an ongoing dialogue with users.
Rebecca Wootton:
“A lot of the people we work with are not technical, so sometimes the idea of moving from a paper process that they’re comfortable with to a digital solution can be challenging for them. The more we keep them involved as we go along the stages, it onboards them better.”
The value of student internships
The development team typically works on three or four new builds each year, with some spanning lengthy timespans.
Five of the six team members, including Web Development Team Leader Rebecca Wootton, have joined via student internships, usually working one day a week until graduation and then returning if and when a vacancy becomes available.
As the scale of projects become bigger and wider ranging the team are looking at more collaborative ways of working to increase their production and portfolio knowledge. Until now, they have often taken on a project and worked on it single-handedly which has both positives and negatives.
Rebecca Wootton:
“Clinicians working with one person that they can create a working relationship with is important. A real highlight of this project has been how our full-stack developer Andrew Pheasey has taken it from start to finish, curating a solution bespoke to the department’s needs and managing that relationship which is something to be very proud of.
He flies under the radar a lot of the time, but he really deserves the recognition. He started with us as a student web developer in 2017, only returning full time in 2019, so it shows what someone can achieve and contribute in a short amount of time.”
What we achieved…
Rebecca Wootton:
“There is no paper used [in this process] anymore. We’ve introduced the system in every one of the 60 wards and departments, audits have been completed in all of them and there’s been no issues. I think it’s a real achievement that we’ve managed to get buy in from everywhere.
We’ll be keeping the learning process going because as people leave and new managers and s come in, they'll have to learn and adapt to this process. As the trust is going more and more digital, I think people are becoming more accepting of these digital procedures.”
Karen Austin:
“Feedback from system users has only been positive; ease of completion, going paperless, time reduction and email reminders have all been viewed very positively. From a personal perspective, Rebecca and Andrew have been a pleasure to work with, fully taking on board the fact that I have never been involved in any project like it before and they would need to use terminology I could understand. Andrew supported me throughout the whole journey which was very much a learning experience for me.
We now have a truly paperless, cost-effective, timesaving, and time-bound process. I look forward to being involved in digitising other paper processes in the future and would encourage others to look at the paper heavy processes they use and consider going digital.”
What’s next?
Rebecca Wootton and her web development team will be working with Karen Austin again on the digitisation of the Patient Group Directorate (PGD) process.
PGDs provide a legal framework that allows some registered health professionals to supply and/or administer specified medicines to a pre-defined group of patients, without them having to see a prescriber.
There can be multiple PGDs in use on wards/departments, for example, the Emergency Department, all of which must be reviewed and signed off by multiple signatories every three years. This is an admin-heavy, time-weighted process as the Pharmacy Administration Assistant must tour the hospitals collecting draft PGDs from several sign-off signatories as drafts were often mislaid or went missing. When this happens, the sign off process had to begin again.
Rebecca Wootton explains:
“All PGDs are reviewed regularly for staff lists and a copy must be kept on the ward and department. A lot of the time in the process is spent by the Admin Assistant taking the PGD to a person’s PA, leaving it with them for a week to get sign-off. They then collect it and repeat the process with the next person on the list.
The digitisation of the process will allow for quick completion of the workflow from start to finish. It will create a central store of all PGDs across the hospitals and provide clarity on their review status. The decrease in administration time will open up resource to focus on other areas of the pharmacy.”
Get in touch
THIS enables new, empowering, efficient, and secure communications and IT services for clients including health trusts, GPs, laboratories, hospices, and care charities. The innovations and collaborations chronicled here are examples of our work with our host trust. It is important to stress however, that our solutions are just as relevant to other trusts and healthcare sectors. If you are interested in working with us, get in touch.
Subscribe to Informatics Insights and Advice
Take advantage of the latest news and information from The Health Informatics Service. Read about our innovative work with healthcare clients across the UK and get our expert insights and recommendations to help and inspire your work.